Weigh the Outrage of the FAA BMI Trigger
The outrage over the FAA’s recently announced medical certification policy to require pilots with a body mass index (BMI) of 40 or more to be examined for obstructive sleep apnea has been consistent across all channels. (And is it coincidence that the FAA implemented it just before Thanksgiving?)
But not one of the chest-thumping screeds has provided an understandable mental image of what a 40 BMI looks like. “Fat” is the most common adjective, but it does not even come close. Try “morbidly obese,” because a 40 BMI is the threshold for this condition. Such pilots would unlikely be able to squeeze into the cockpit let alone the pilot’s seat.
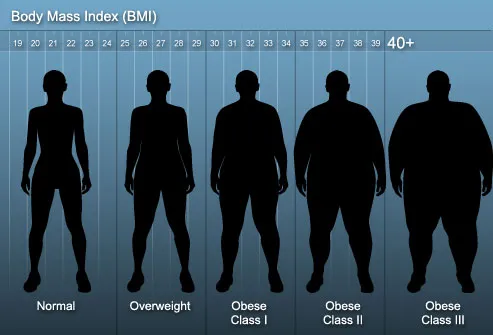
Let’s put it another way. What is your BMI, your ratio of height to weight? If you don’t know, here’s the link to a calculator. Now, keep adding weight until your BMI reaches 40. How much will you weigh? At 6-foot-5 and 240 pounds, my BMI is 28.5.
The normal BMI range is 18.5 to 24.9. Like many of my age, my BMI is in the “overweight” category, which starts at 25, and it is 1.5 points shy of obesity’s doorstep. And it’s not even close to the FAA’s 40 BMI trigger. To reach that I’d have to push the scale to 340 pounds. A 6-footer would weigh 295 pounds.
When was the last time you you saw a pilot of this size getting in or out of an airplane? So why is everyone giving the impression that the requirement imposes dire consequences on all overweight aviators? Let’s be honest here, many other obesity-related conditions rank higher on the medical certificate denial list.
Listing the health conditions related to obesity, University of Rochester Medical Center starts with Type 2 Diabetes and high blood pressure before it gets to joint problems, sleep apnea, acid reflux, depression, infertility, and incontinence. If there’s a list that motivates the proper combination of diet and exercise, this is it.
In his editorial discussing the new policy, Federal Air Surgeon Fred Tilton said the BMI trigger would, in time, be lowered, “once we have appropriately dealt with every airman examinee who has a BMI of 40 or greater.” When that will be is anyone’s guess, but what I’d really like to know is how many applicants have reached this register? Maybe most of them are air traffic controllers, to whom the new policy also applies.
 More intriguing are Tilton’s words encouraging AMEs to be on the lookout for other sleep-related disorders, “such as insomnia, parasomnias, or restless leg syndrome; or other physical anomalies such as a retrograde mandible, a large tongue or large tonsils, or neuromuscular or connective tissue disorders, because they could also be signs of problems that could interfere with restorative sleep.”
More intriguing are Tilton’s words encouraging AMEs to be on the lookout for other sleep-related disorders, “such as insomnia, parasomnias, or restless leg syndrome; or other physical anomalies such as a retrograde mandible, a large tongue or large tonsils, or neuromuscular or connective tissue disorders, because they could also be signs of problems that could interfere with restorative sleep.”
Some have rightly said that BMI is an imperfect measure, that fits individuals, such as NFL players, have higher BMIs because muscle weighs more than fat. True enough. Take, for example, the late, great Reggie White. At 6-foot-5 and 300 pounds, his BMI was 35.6, still well under the FAA trigger. And Reggie died from cardiac arrhythmia aggravated by sleep apnea.
Lest you think I care naught for the obese, until a month ago, I was—by my BMI—one of them. But thanks to my new doc, who this last January presented the consequences of obesity in terms that resonated with me, diet and exercise have trimmed 25 pounds from my BMI, moving me into the overweight category. And I have another 25 to go.
Ultimately, what bothers me most about the outrage against the FAA’s BMI trigger is that almost everything I’ve read about it strongly suggests that commenters jumped on their online soapboxes without thinking things through. I think most pilots will agree that in flight, acting before thinking often leads to an undesirable outcome.
And then there are the social implications. When the financial costs imposed on those who suffer from the medical conditions associated with morbid obesity is more important than their quality—or continuance—of life, what does that say about our concern for the family of aviators?

Are You a Space Geek?

